Harriet the Spy is the Reason I Eat Tomato Sandwiches
When I saw a headline that said this was the best tomato sandwich ever, I had to try it. I think they may be right. Totally worth trying while tomatoes are in season! Link to the recipe from the New York TImes
This tree is a short 5 minute walk from the Children’s Hospital of New Orleans, which made it easy to walk there if I had a break in the middle of the day to connect with history, nature, and spirit.
Old trees exist everywhere… Find one near you (or when you travel). #Awe
My father used to tell me if you got one good idea out of a book it was worth reading it. I just came across this image in Austin Kleon’s blog… Creating the cards (and taking the photo) surely helps remember important ideas (and where they came from).
Although I follow my ancestors’ spiritual path, I have incredible respect for the varied traditional paths my friends follow…and for those who follow no specific spiritual tradition. This post, which is the text of a sermon I gave on Sunday, does not and should not imply anything beyond my desire to share… and to lift up love where ever we find it.
Nadia Bolz-Weber, one of my favorite modern theologians, is quoted as having said that “reading parables is like using riddles to get directions to the airport.”
Today we have a parable trying to metaphorically get us to our flight on time…and we have a passage that explains why Jesus spoke in parables in the first place, an explanation that was added later by leaders in the early church. (Which is why I’m choosing to focus on the first part, the words of Jesus).
That same day Jesus went out of the house and sat beside the sea. Such great crowds gathered around him that he got into a boat and sat there, while the whole crowd stood on the beach. And he told them many things in parables, saying: “Listen! A sower went out to sow. And as he sowed, some seeds fell on a path, and the birds came and ate them up. Other seeds fell on rocky ground, where they did not have much soil, and they sprang up quickly, since they had no depth of soil. But when the sun rose, they were scorched, and since they had no root, they withered away. Other seeds fell among thorns, and the thorns grew up and choked them. Other seeds fell on good soil and brought forth grain, some a hundredfold, some sixty, some thirty. If you have ears,hear!” Matthew 13:1-9
Soil, Seed, and Sower.
Those are the three obvious things that could be starting points to understand the meaning of this parable.
The soil is where most of us start … But I’m becoming more and more convinced that soil may be the least important of the three symbols here (despite what those early church leaders added in their explanation). That is contrary to what most of us have been taught about this parable. Most people interpret the parable of the sower as a directive to figure out if we, in our own lives, are the hard soil, the gravel, an unkept patch of weeds, or good soil… whether or not we prepared the soil of our souls so that when God’s seeds land there they can grow.
The seeds that are being sown are the second powerful symbol. This seems fairly straightforward…Most scholars agree, and most of us have been taught, that the seeds in this parable are a metaphor for the words of God, a metaphor for planting something new, something good, something of God.
But let’s not forget – this is called the Parable of the Sower… not the Parable of the Soil or the Parable of the Seeds. It’s not set up to primarily be a lesson about the kind of soil you are, or the seeds being planted in your heart.
And more specifically, let’s talk about sowing 2000 years ago, when Jesus spoke these words. Sowing in 1st century Israel wasn’t anything like how farmers today plant their crops – and that’s important to understand this verse.
Modern farmers plow their fields and then plant the seeds, but in 1st century Israel it was the opposite… first the seeds and then the plow.
Sowing took place after the first big rain of the year in October or November, a rain that softened the ground that had been baked during the summer…which is mentioned in today’s reading from Psalm 65:
Thus have you prepared the land: drenching its furrows, breaking up its clods, softening it with showers, blessing its yield.
Following the first rain of autumn, farmers would walk with a bowl of seeds, reaching in to grab handfuls of seeds to fling in arcs over the ground. (This technique, by the way, is called broadcast sowing – which is the origin of the word broadcast used to describe spreading things by radio or TV.)
The seeds were tossed onto fields that had been basically untouched since the harvest in May, 5-6 months before. During those fallow months, people walked across the fields, tamping down the earth as they walked which created paths. Seeds that fell on these paths were easily seen and quickly eaten by birds.
After the seeds were scattered they plowed, which ensured that at least some, if not most of the seeds were covered. And then they did something that is truly not part of modern farming. They used oxen or other animals – and their own feet – to walk over the entire surface of the field to push seeds left on the surface into the ground. Which led to three possible outcomes for the seeds that hadn’t been eaten by the birds:
If the seeds ended up in shallow ground that couldn’t be plowed because of rocks or gravel, they would grow, but not have enough roots to live.
If the seeds were in a part of the field where weeds had been plowed under but not uprooted, the weeds would take over and choke growth from the seeds.
And then there’s the third possible outcome – In the parts of the field where everything worked – where the seeds were covered, the soil was deep enough, and there weren’t any weeds, you could expect them to grow and produce a harvest.
All that to say… It’s clear that these farmers lost a lot of seeds… to birds, to shallow ground, to weeds. But “losing” all these seeds was normal and expected… It was part of farming in the 1st century. It’s still part of gardening and farming now – as reflected in a proverb often used to teach young gardeners and farmers: “One for the mouse, one for the crow, one to rot, one to grow”.
That’s why I think this isn’t a parable about the soil or the lack of preparation of the field. It’s not about our hard hearts, or weed filled spirits, or being shallow. Because everything about how these seeds were planted and how they were expected to grow (or not) was normal operating procedure for a 1st century farmer.
What isn’t particularly normal or expected is the harvest that Jesus predicts for the seeds that grow well. Everyone who heard his words in the 1st century would have known that a reasonable harvest would give you seven times what you planted. A truly exceptional harvest would be ten-fold. But Jesus talks about thirty, sixty, a hundred-fold! Everyone listening would have known that was impossible, that he was talking about something miraculous.
So why parables? Why this parable?
Like last week, there is a clue in the passage left out of today’s Gospel text. In verse 13, Jesus says “The reason I speak to them in parables is that ‘seeing they do not perceive, and hearing they do not listen, nor do they understand.’”
This seems crazy, right? What he’s saying here is “I am telling them these weird stories, these parables, because if I just tell them what to do, they won’t get it.”
Why not just tell us what to do? Why do we have to ponder these “riddles”? The best explanation I’ve found so far comes from Rachel Held Evans…
“In Walking on Water, Madeleine L’Engle tells of a young woman who told the author, “I read A Wrinkle in Time when I was eight or nine. I didn’t understand it, but I knew what it was about.”
That’s often how I feel about the parables of Jesus. I don’t understand them exactly, but I know what they’re about.
L’Engle concludes: “…One does not have to understand to be obedient. Instead of understanding—that intellectual understanding which we are so fond of—there is a feeling of rightness, of knowing, knowing things which you are not yet able to understand…As long as we know what it’s about, then we can have the courage to go wherever we are asked to go, even if we fear that the road may take us through danger and pain.”
So here’s what I think this parable is about, which is more important than trying to intellectually understand it:
God throws the seeds we need into the world with almost reckless abandon and without judgement. God knows that only a few will take root… that’s the nature of sowing seeds! But when they do take root and grow – in us, in our communities, and in our world, what happens is beyond what we can imagine, each seed that takes root producing a miraculous number of new seeds for us to sow into the soil of our injured and hurting world.
This parable is also about our responsibility as sowers. It tells us that we aren’t responsible for what happens to the seeds of love we sow in the world…But we have a responsibility, a duty to sow them anyway, flinging them with reckless abandon and without judgement, knowing that only a small portion of them will take root.
This parable is also about what happens when God’s love takes root, how that love multiplies and grows in ways we can’t imagine.
We don’t have to understand this parable to be obedient – because we know what it’s about.
So load up your shoulder bags and let’s go.
It’s time to sow some seeds.
Amen.
Sermons are meant to be heard. If you’d like to listen to this one, it starts at 31:26 here.
Radio Garden. This amazing website lets you spin a globe to randomly land on live FM stations over the entire planet. So cool.
Check Your Instagram Settings!
This seems important. You can read more about it here, but Meta’s new stealth policy sounds particularly dangerous for physicians and other healers.
“All someone has to do is tag your account’s profile in a prompt—if it’s public—and they can use Meta AI to generate an image using your likeness.”
Here’s how to tune this off..
“Open the Instagram app, tap your profile, and then tap the three lines in the top-right corner of the screen. Then, scroll down to the Sharing and reuse tab. Here is where you should see a section labeled Allow people to use your content on Instagram and with AI features on Meta, with a toggle for Posts and one for Reels.”
Mighty Fungi
AM (arbuscular mycorrhizal) fungi were in the news last week because of a beautiful study that determined there are “621 trillion miles of fungal pathways containing around 300 megatons of carbon within Earth’s topsoils”.
“The answer is not to abandon fertilizers but to find a balance between fertilizer use and nurturing the living soils and the billions of microbial communities that quietly sustain American and global agriculture.”
AM fungi is a really good example of something very small and quite amazing that I’ve never paid attention to before. Good lesson.
Our goal should be to live life in radical amazement…to get up in the morning and look at the world in a way that takes nothing for granted. Everything is phenomenal;everything is incredible;never treat life casually. To be spiritual is to be amazed.
Although I follow my ancestors’ spiritual path, I have incredible respect for the varied traditional paths my friends follow…and for those who follow no specific spiritual tradition. This post, which is the text of a sermon I gave today, does not and should not imply anything beyond my desire to share… and to lift up love where ever we find it.
“But to what will I compare this generation? It is like children sitting in the marketplaces and calling to one another,‘We played the flute for you, and you did not dance; we wailed, and you did not mourn. For John came neither eating nor drinking, and they say, ‘He has a demon’; the Son of Man came eating and drinking, and they say, ‘Look, a glutton and a drunkard, a friend of tax collectors and sinners!’ Yet wisdom is vindicated by her deeds.”
At that time Jesus said, “I thank you, Father, Lord of heaven and earth, because you have hidden these things from the wise and the intelligent and have revealed them to infants; yes, Father, for such was your gracious will. All things have been handed over to me by my Father, and no one knows the Son except the Father, and no one knows the Father except the Son and anyone to whom the Son chooses to reveal him.”
“Come to me, all you who are weary and are carrying heavy burdens, and I will give you rest. Take my yoke upon you, and learn from me, for I am gentle and humble in heart, and you will find rest for your souls. For my yoke is easy, and my burden is light.” Matthew 11: 16-19, 25-28
This week’s Gospel reading is a complicated but rich text, particularly if we take on the challenge of trying to really understand what Jesus is teaching here.
At the time he delivers this lesson, Jesus has finished his instruction of the disciples, delivered the sermon on the mount, and has started to travel to different cities to teach and proclaim his message. Things are getting a little intense… John the Baptist is in prison, and Jesus is starting to be labelled as a trouble maker by the authorities.
The verse has three parts that at first don’t seem that connected… It starts with children in a marketplace, moves to infants who are wise, and ends with yokes and heavy burdens.
The first part of the verse, the children in the marketplace, starts with this: “What comparison can I make with this generation? They are like children shouting to others as they sit in the marketplace, ‘We piped you a tune, but you wouldn’t dance. We sang you a dirge, but you wouldn’t mourn.’
I had a lot of questions after reading this, but the biggest one was this: Who is Jesus talking about when he says “this generation”? Who are these people Jesus compares to children (and not in a good way) who refuse to participate, who reject the other children inviting them to take part in the joy of dancing and the grief of mourning?
The verse continues with this: For John came neither eating nor drinking, and they say, ‘He is possessed.’ The Chosen One comes, eating and drinking, and they say, ‘This one is a glutton and a drunkard, a friend of tax collectors and sinners.’
John was an ascetic. He fasted and lived without other comforts for spiritual reasons. But what’s important for our understanding of this verse is that the prophecy he proclaimed was a threat to the status quo, to the power of the religious leaders of the time. So they declared his fasting as a sign he was possessed by a demon.
Jesus wasn’t an ascetic. He loved a good meal and no matter what table he sat at, everyone was welcome. But they didn’t like that, either… so they called him “a glutton and a drunkard, a friend of tax collectors and sinners.”
From this we know that “this generation” doesn’t join in when they are invited to dance and mourn… and not only do they refuse that invitation, they badmouth the people inviting them. But we still don’t know exactly who “this generation” refers to because it’s left intentionally vague. Jesus doesn’t specifically call out the religious leaders who were protecting their religious authority. He also doesn’t call out the followers who went along with those leaders because they thought the way of least resistance was easier.
He just says “All y’all” (which means we are included) by referring to them as “this generation”.
The take home message here is that the religious leaders, political officials, and people who just wanted to keep their heads down to avoid trouble didn’t want to have anything to do with John and Jesus… because the message they were spreading was dangerous. It threatened to overthrow the status quo, to pull the rug out from under power… their power.
You’ll notice there is a gap in the gospel reading today… verses 20-24 aren’t included. I won’t read them all, but I think Verse 20 is important: Then [Jesus] began to reproach the cities in which most of his deeds of power had been done, because they did not repent.”
Let’s read that again – Then [Jesus] began to reproach the cities in which most of his deeds of power had been done, because they did not repent.”
It’s right there! Jesus’ acts of healing, teaching, and caring were “deeds of power”. That’s why the folks in power were so afraid of Jesus, why they slandered him, and why – ultimately – they crucified him.
But here’s the punch line, how Jesus ends his teaching about “this generation”… After he describes the slurs being used against John and himself, after he shakes his head at the “children” in power who were not understanding what was happening, he says this: “Yet wisdom is vindicated by her deeds.”
But he leaves us hanging… He doesn’t explain what that means. He doesn’t tell us who wisdom is (although we suspect it is Jesus). No, the next thing that happens is that he prays…
Then Jesus prayed, “Abba God, Creator of heaven and earth, to you I offer praise;for what you have hidden from the learned and the clever, you have revealed to infants.
Unattributed photo from TikTok
An hour or two after a healthy baby is born, there is a magic hour or so where they behold the world they have arrived in. For that hour, they are wide-eyed and have an extraordinary expression on their face that is a combination of wonder, curiosity, and deep peace. They look around as if they can’t believe the wonder of what they are seeing, of this gift they have been given. I’ve never seen that expression on any other human face, of any age. (The closest I’ve ever seen is the face of the Dalai Lama and his friend Bishop Desmond Tutu when they are laughing with each other, but even then – it is not the one time holy gaze of a newborn infant.)
I don’t think we have words to describe the wisdom Jesus is talking about in this verse.
I don’t think it’s verbal at all.
But I think we all know it.
I think the wisdom Jesus is referring to is given to us when we are born, a wisdom that is reflected in the brief moment of wonder when we behold the world around us with inexplicable joy, as we experience God’s unforced rhythms of grace for the first time.
This gift of wisdom isn’t just a birth-day present, we all still have it. This gift, this grace, is within each of us at all times and in all places… we just have to remember that it’s there, a gift from the Holy Spirit.
It’s this particular kind of wisdom, this grace, that I think is the focus of the last part of today’s reading.
Come unto me, all ye that labour and are heavy laden, and I will give you rest.
Take my yoke upon you, and learn of me; for I am meek and lowly in heart: and ye shall find rest unto your souls.
(Sometimes the poetry of the King James Version is just what the occasion calls for.)
Last week we had a special service to guide us in the practice of lamentation. We lamented together, and we learned about the need to bear witness to the heaviness we all carry, especially in these times.
When we hear the word “yoke” we appropriately think of the heavy wooden crossbeam used to attach two oxen together, to let them pull a heavy load together…
There have been so many days I had to lean on this verse… The days I had hard conversations with grief filled parents, the days I was so exhausted I didn’t know if I could carry on… But even then, even when I found solace in these words, I couldn’t help but wonder….. Why, if I’m already carrying a heavy load, would the answer be to add more weight to my shoulders? Why would I want to add a yoke, even if it was the yoke of Jesus?
The answer to that question is (literally) lost in translation.
In the 1st century, when Jesus spoke these words in Aramaic, when he told his followers “Take my yoke upon you” it had a much deeper meaning, one that they would have all known… because the word Yoke referred to the teachings of a Rabbi, the specific way a rabbi guided you in the “difficult but joyous task of obedience to the Torah”.
Every rabbi had their own yoke, their own unique interpretations and teachings that their students were expected to live by… and Jesus was no different.
What was different was how he described what we can expect if and when we take his yoke upon us.
Take my yoke upon you, and learn of me; for I am meek and lowly in heart: and ye shall find rest unto your souls.
Jesus says “follow me” at least 12 times in the Gospels. I’ve always seen that in my head as like following someone on rounds in the hospital (sorry, but it’s true)… walking physically behind them, trying to follow in their footsteps, having them lead me to the next place I need to go.
Eugene Peterson’s translation helps us better understand this verse and what it really means to follow Jesus… what it means to put on his yoke: “Walk with me and work with me—watch how I do it. Learn the unforced rhythms of grace.”
Today’s gospel lesson comes down to this:
Following Christ doesn’t mean what we usually think of when we say we are going to follow someone. It’s not about traveling behind Jesus, walking in his footsteps, having him lead the way…
Following Christ means walking with him, beside him in lock step – because we are yoked to him.
Following Christ means working with him to help co-create God’s kindom on earth.
Following Christ means watching him, learning from him, imitating him … in other words, striving to be true disciples of Christ.
Dr. Roger’s team custom engineered grass for every stadium (including the indoor NFL stadiums that have never had grass on the field) which was grown on different sod farms in the United States and shipped to the stadiums in the last few months.
Seeing the world through food… (at least 48 countries in the World)
“I can’t really saywhy I decided to cook, or otherwise procure, a dish representing every nation at the World Cup, except that I thought it might be kind of fun…”
Tim Murphy
In this article Tim Murphy recounts his family’s attempt to cook (or procure) food from each of the 48 countries “by eating, more or less in order, through the 12 groups of four teams who will meet in the tournament’s opening rounds.” The Houston Chronicle made it easy for those of us who live in Houston by creating a list of 48 restaurants where you can find the cuisine of the competing countries. And check out this blog that teaches kids why cooking is a lot like playing soccer!
On a more gentle note, I was touched by two different stories I read this week, both having to do with grief and the wind.
A little over 25 years ago Gus Guadagnino hung a windchime from a tree on the property he owned adjacent to the Suncoast trail near Spring Hill, Florida in memory of his mother. Other folks did the same and now there are over 100 different chimes hanging from the tree.
It must be a incredible experience to stand under this tree on a windy day…
The second story was about “wind phones”, old fashioned, disconnected, rotary phones placed in isolated, natural places that people use to “talk” to someone they have lost.
“Here they can say the things left unsaid. Wind phones offer a setting for the person to tell the story of their grief, to reminiscence and to continue to connect to the person who is gone.”
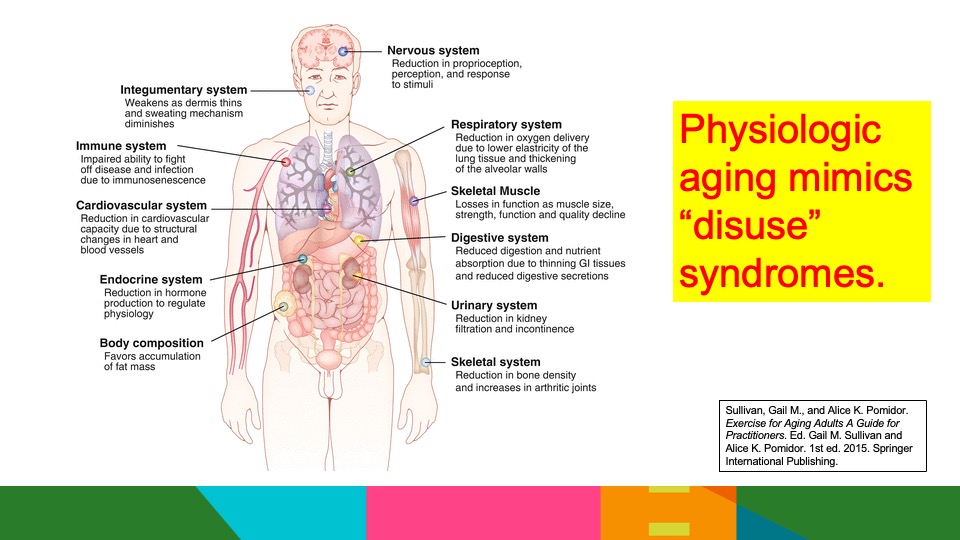
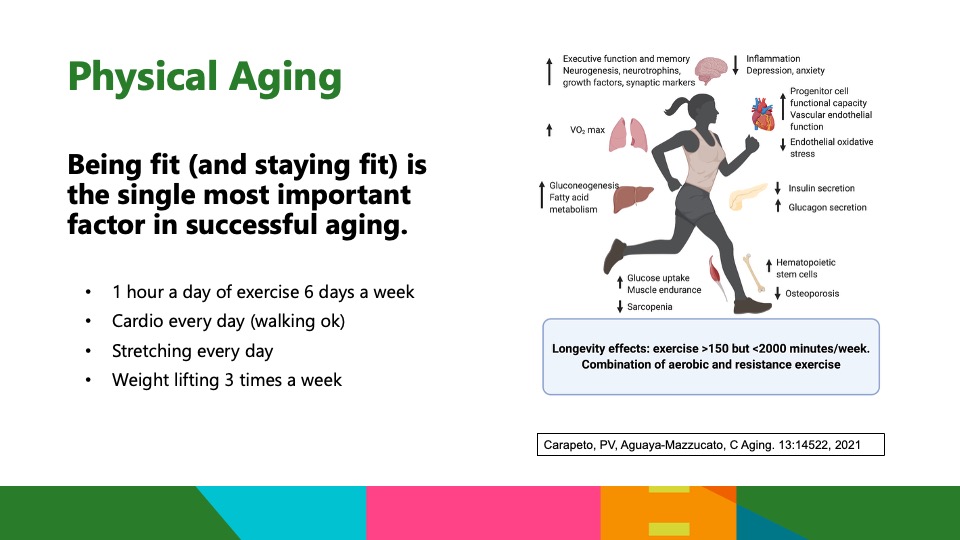
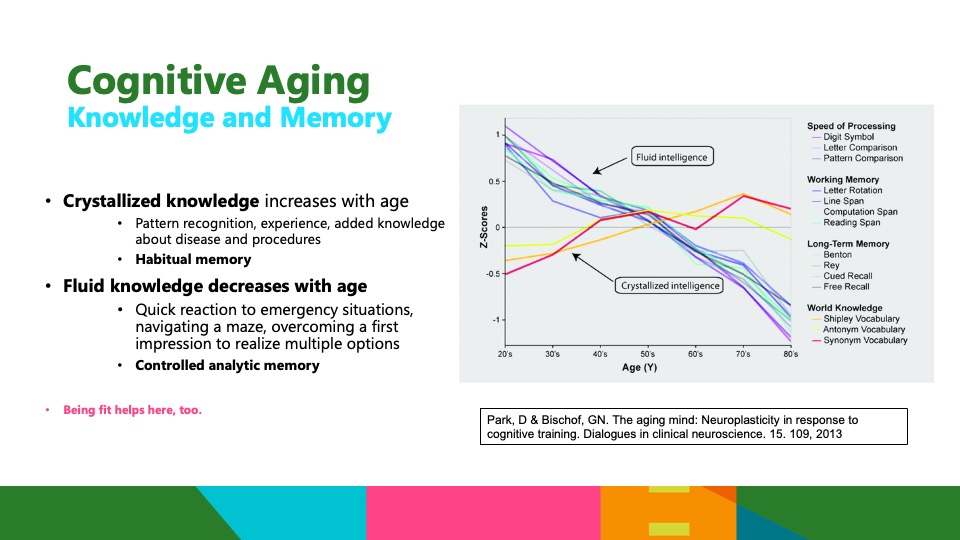
I was asked to give a talk with this title several years ago for the annual meeting of the American College of Surgeons. I was surprised at the enthusiastic response then, and more surprised at how many times other folks have asked me to talk about this topic since. I had a friend recently ask me if there was a link to the talk that they could share with others. It wasn’t recorded (that I know of), so I’m posting the slides here. I think they are mostly self explanatory, but if you have any questions, please let me know!
I hope it’s still true, but for many years the neurosurgery service at the hospital where I worked had a wonderful ritual. Every time a neurosurgery resident performed a case for the first time, they were sent to the cafeteria to buy ice cream for the entire team.
Ice cream (especially Blue Bell Vanilla…. IYKYK) is joy in a container, joy that can be expanded by using the simple and ancient practice of a blessing. Judaism has a long history, and many resources for blessing the routine moments in life, including a blessing for the first time something is experienced. You don’t have to be religious to adopt this practice – you just have to find how to acknowledge and appreciate the moments that inspire joy, awe, and wonder.
The power of this practice is amplified by writing them down, which is why I think it’s important for everyone learning to be a healer to keep a journal. There are many reasons a journal helps make sense of your experiences, but being able to relive these “first time” experiences years in the future will surprise and sustain you in ways you can’t imagine now.
So spend a few moments recording what happened, who was there, and how you felt the first time you hear a murmur, the first time you cry with a patient, the first time you see the miracle of birth, and the first time you bear witness to a family’s unimaginable loss. Look for first times that maybe aren’t so obvious, too, like the first time you meet a famous teacher, the first time you walk into a new hospital, the first time you get to park in the “good” parking spaces.
But most of all, record the moments you never want to forget… like the first time you hold a newborn during the magic hour when they are starstruck, looking around with open eyes and wonder (the most peaceful expression you will ever see on a human face).
So buy the ice cream for the first case.
And then … write down how blessed it made you feel.
Instructions for living a life: Pay attention. Be astonished. Tell about it.
Merriam-Webster defines a polymath as “a person of encyclopedic learning”, but that doesn’t seem to really convey the wonder of a true polymath.Because polymaths (at least the ones I’ve met) not only know a lot about a variety of topics, they are also passionate about them. You never feel that they have an obligation to study or a “goal” to learn…They usually convey a joy of learning (combined with extraordinary intellect) that leads them to their “encyclopedic learning”.
The universe is flat and may be shaped like a Pringles chip
This article explains why cosmologists (who study the cosmos, not makeup) are sure that the universe is flat. What they aren’t sure about is which of the 18 possible 3D flat shapes best fits what they currently understand about the universe.
Caffeine is a pleasure and, for many, almost a necessity. But caffeine can be a double-edged sword if you don’t understand how to use it to help with fatigue, sleepiness, and a need to study for exams!
Although this piece is directed primarily at medical students and residents, the information applies to everyone who uses caffeine to stay alert.
Disclaimer: Although I still follow my ancestors’ spiritual path, I have incredible respect for the varied traditional paths my friends follow…and for those who follow no specific spiritual tradition. This post, which is the text of a sermon I gave today, does not and should not imply anything beyond my desire to share… and to lift up love where ever we find it.
When the day of Pentecost had come, they were all together in one place. And suddenly from heaven there came a sound like the rush of a violent wind, and it filled the entire house where they were sitting. Divided tongues, as of fire, appeared among them, and a tongue rested on each of them. All of them were filled with the Holy Spirit and began to speak in other languages, as the Spirit gave them ability. Now there were devout Jews from every people under heaven living in Jerusalem. And at this sound the crowd gathered and was bewildered, because each one heard them speaking in the native language of each. Amazed and astonished, they asked, “Are not all these who are speaking Galileans? And how is it that we hear, each of us, in our own native language? Parthians, Medes, Elamites, and residents of Mesopotamia, Judea and Cappadocia, Pontus and Asia, Phrygia and Pamphylia, Egypt and the parts of Libya belonging to Cyrene, and visitors from Rome, both Jews and proselytes, Cretans and Arabs—in our own languages we hear them speaking about God’s deeds of power.” All were amazed and perplexed, saying to one another, “What does this mean?” But others sneered and said, “They are filled with new wine.”Acts 2:1-13
Artist unknown
Today is Pentecost Sunday, which marks the end of the Easter celebration and the beginning of what we call “Ordinary Time” in the church’s calendar.
(By the way, that’s ordinary as in ordinal… days we count…. Not ordinary as in mundane)
The first half of the liturgical calendar tells the story of Jesus – starting with Advent and ending today, with Pentecost. The second half, which starts tomorrow, tells the story of the people of God, the story of the community of believers that was born on Pentecost over 2000 years ago.
Before we enter Ordinary Time, we leave the Easter season with (literally) a bang… with wind and fire.
Let’s listen to today’s lesson again, this time from Eugene Peterson’s translation of the Bible…
When the Feast of Pentecost came, they were all together in one place. Without warning there was a sound like a strong wind, gale force—no one could tell where it came from. It filled the whole building. Then, like a wildfire, the Holy Spirit spread through their ranks, and they started speaking in a number of different languages as the Spirit prompted them.
There’s a lot to unpack here, but let’s start at the beginning… “They were all together”…
Who is “they” and why were they all together?
A little further in Chapter 2 of Acts, Luke tells us who “they” refers to. It’s the 12 disciples plus 120 other people who became believers because they had seen the risen Christ during the 40 days he walked among them.
So that’s who “they” refers to… but why were they all together?
The word Pentecost is derived from the Greek Pentakonta, and means “fiftieth”.
“Pentecost” is the Greek word for Shavuot, the Jewish festival that celebrates the gift of the first fruits of the harvest and the gift of being given the Torah at Mount Sinai. It’s a festival that happens 50 days after Passover (hence “Pentecost”). Pentecost, like Passover, was a pilgrimage festival – which meant everyone travelled to be together to celebrate. That’s why they were all in one place, to celebrate Pentecost… that and the fact that 10 days earlier, at the time of his Ascension, Jesus had told them not to leave Jerusalem.
It had been only 50 days since Jesus’ execution.. But the 12 disciples and the 120 new followers weren’t grieving…
They knew Jesus was alive, raised from the dead…Because for 40 days after his resurrection Jesus appeared over and over to not only the disciples but to many others. Scripture tells us that he appeared to more than 500 people on one occasion (1 Cor 15:6) and that he gave “convincing proofs to many other people” (Acts 1:3)
At the end of those 40 days, 10 days before the festival of Pentecost, Jesus ascended into heaven… but not before preparing his followers for what would happen on Pentecost.
“When they were together for the last time they asked, “Master, are you going to restore the kingdom to Israel now? Is this the time?”
Jesus answered, “You don’t get to know the time. Timing is the Father’s business. What you’ll get is the Holy Spirit…”The Message
Which brings us to the bang… the wind and fire
I suspect you learned the weird math of Western Christianity like I did. You know… the 1+1+1 equals 3 which equals 1? It didn’t make sense then, and it’s still hard to understand for me now.
Let me share some thoughts from Richard Rohr that may help:
Not exactly One, Christian mystics and teachers attempt to explain, and yet perfectly One; not exactly Three but yet Three… No wonder it took us three centuries to even find a word to describe such a nonsensical image of God. Note this for now: the principle of one is lonely; the principle of two is oppositional and moves you toward preference; the principle of three is inherently moving, dynamic, and generative.
One is lonely. Two makes you choose. Three is a community.
The mystery of the Triune God helps us understand that God is not “something or someone”, God is community, relationships, connection… “inherently moving, dynamic, and generative.”
Richard Rohr also reminds us that when we try to describe God, Christ, Holy Spirit, or even Love with words, we will never do it well. As he puts it “All theological language is an approximation, offered tentatively in holy awe.”
All theological language is an approximation, offered tentatively in holy awe.
richard rohr
It’s so hard to come up with words that let us grasp mystery… so we use images and metaphors. We talk of wind, fire, and water… as we grasp at trying to understand the majesty and mystery of a triune God.
God for us, we call you [Creator] God alongside us, we call you Jesus God within us, we call you Holy Spirit
richard rohr
Which brings me back to today’s scripture…
Without warning there was a sound like a strong wind, gale force—no one could tell where it came from. It filled the whole building. Then, like a wildfire, the Holy Spirit spread through their ranks, and they started speaking in a number of different languages…
God-within the disciples and those who had seen the risen Christ was ignited and “spread like wildfire”. God-within spilled out in the words they spoke… and not just any words – words in a number of different languages…Words that let everyone there hear the Good News in their own language.
Words that let them understand.
Words that connected each one of them to each other and the mystery of Divine Love.
It was so loud, so crazy, that the people who ran towards them to see what was going on thought they were drunk.
Today’s verse is followed by a sermon by Peter explaining that these people weren’t drunk… they were fulfilling prophesy. He walks them through the prophesy and then retells the story of the execution of Jesus on the cross and his resurrection from the dead, ending with “Therefore let the entire house of Israel know with certainty that God has made him both Lord and Messiah, this Jesus whom you crucified.”
We are then told that the people listening to Peter were “cut to the heart.” and began to beg him to tell him what they should do.
He told them to repent and be baptized.
The text continues with these words… “They were convinced by his arguments, and they accepted what he said and were baptized. That very day about three thousand were added to the number of those converted.”
The Church was born.
There have been ~70 generations of human beings since that moment.
Which means..
It is highly probable that one of your biological ancestors was there…
And it is certain that at least one of your spiritual ancestors was there.
…Because we are part of an unbroken chain of spiritual inheritance kept vital and alive by the roaring wind and tongues of fire of the Holy Spirit present within us and around us … then, now, and always….
God for us, we praise you and call you [Creator]
God alongside us, we praise you and call you Jesus
God within us, we praise you and call you Holy Spirit
And all God’s people say…
Amen
Claire Tabouret’s design for one of six stain glass windows depicting Pentecost for Notre-Dame cathedral
Sermons are meant to be heard. If you’d like to listen to this one, it will be posted here.
ACHOO may be one of the best acronyms for a physiologic condition I’ve ever seen. It stands for Autosomal Dominant Compelling Helio-Ophthalmic Outburst. The ACHOO syndrome refers to the inherited trait of sneezing when you are suddenly exposed to bright light (like walking outside into bright sunlight). It’s also called photoptarmosis (from the Greek phōs, “light” and ptarmós, “sneeze”)
El Niño is the name given to powerful shifts in Pacific Ocean winds and water temperatures that can drastically transform global weather patterns. Over the centuries these natural patterns have sparked epic droughts and heat waves, and have intensified epidemics.
I cooked this recipe for the first time this week and, in keeping with my promise to add more topics to support students, residents, and busy docs, decided it was worth sharing. Start with the basic recipe and then change it to your taste (I’m adding some whole almonds and cashews next time).
Take a bag of this granola with you when you are on call to mix with yogurt – or just grab handfuls when you need some healthy calories.
p.s. I substituted olive oil for the vegetable oil which was delicious and probably a little healthier
p.p.s. If you do the math, this is incredibly cheap compared to commercially made granola, granola bars, or other grain based snacks
p.p.p.s I have used #CallFood for years on social media (Bluesky,Facebook, and Instagram) as a hashtag for recipes that don’t take long to cook, taste great, and are healthy (In case you are looking for more suggestions.)

















































{kind=link}