
I’ve started a new practice as a medical educator that has been working so well that I thought I should share it.
Once (or twice) a day in every teaching hospital every service makes rounds and, while managing and treating their patients, the attending (and/or senior residents) teach.

Inevitably, there are unanswered questions that come up as we discuss patients. Many of them are questions I don’t know the answer to, or are related to a hot topic that might have new information just published. Here are some examples of questions that have come up on rounds on our pediatric surgery service:
- Are there new recommendations about how to manage gallstone pancreatitis and/or choledocholithiasis in kids?
- What is the caloric content of the different formulas we prescribe?
- What is the best way to calculate calorie needs for a burn patient?
- How and why do you swaddle a baby?
- How do you manage supplemental oxygen after you extubate a patient with severe facial burns?
- Where does “second line” come from?
Typically in the past, each student and intern would be assigned one or two of these questions to answer. They would be expected to report back to the team the next day – which might or might not happen depending on how busy the day was (and if the attending remembered to ask them). But to be honest, this way of teaching has become harder with time. There is a post-call resident who is not there the next day, the students often have didactic sessions that are required so they aren’t there, and the day can get so busy that there isn’t (perceived) time to teach on rounds.
But it’s our responsibility to teach (the word doctor means teacher!). Teaching is also a powerful antidote for burnout because its so important and so meaningful. It was clear – I had to come up with a way to make this work in spite of the limitations created by our schedules and clinical responsibilities. So here is what I do now in addition to teaching on rounds:
- During rounds we come up with one question per person (everyone, not just the students and interns).
- Each person is responsible to answer their question via a group email that, as the attending, I start on the first day I’m rounding.
- The answers are short and helpful – as though each person is taking notes for themselves. No PowerPoint presentations, no extensive diatribes.
- The email answer is due before the next morning… but no one is allowed to stay up late to do this.

Here’s what was sent on our group email to answer the examples I listed above. (Disclaimer – These are unedited. Don’t use these for patient care unless you look things up yourself!):
What is the “board answer” for treatment of gallstone pancreatitis?
- Usually mild as the stones pass spontaneously in the majority of patients but can be severe (even life-threatening) although this is rare. This is due both to fluid loss (equivalent of a severe burn) and to SIRS
- initial Tx: Fluid resuscitation, pain control, nutritional support (oral when patients are subjectively hungry – low fat diet)
- Surgery during the same hospitalization (Munoz, 2022) (Berger, 2020) (Noel, 2018)
- ERCP only if there is cholangitis or persistent cholestasis (Schepers, 2020)
What is the “board answer” for treatment of choledocholithiasis.
- First step: Is it asymptomatic or symptomatic (i.e. pancreatitis, cholecystitis, cholangitis)?
- Emergency ERCP (<24hrs) for cholangitis, cholecystitis and/or pancreatitis with obstruction
- Stones must be cleared. There is no benefit to waiting and there is a downside to waiting since there is always a risk of cholangitis or pancreatitis with a stone in place.
- Most surgeons use pre-operative ERCP for known choledocholithiais followed by cholecystectomy, but ERCP at the time of cholecystectomy in adults (Rucci, 2018) (Cianci, 2021) and kids (Fishman, 2020) has been shown to be safe – and perhaps better.
Calorie content of available Tube Feed/Supplements:
Two Cal HN – 2 Calories/mL – high protein
Glycerna 1.2 – 1.2 Calories/mL – lower glycemic index
Nepro Carb Steady – 1.8 Calories/mL – high fiber, gluten free, for lactose intolerant
Impact Peptide 1.5 – 1.5 Calories/mL – supposedly decreases risk of enteral infection in surgical/trauma patient with peptide formulation
Vital 1.2 – 1.2 Calories/mL with 1.2g of NutraFlora per 8oz for gut health
Pediasure Peptide 1.5 – 1.5 Calories/mL – designed for those with malabsorption
Ensure Plus – 1.5 Calories/mL with 16g protein
Osmolite 1.5 – 1.5 Calories/mL – fatty acids for different digestive profile
Jevity 1.2 – 1.2 Calories/mL with 4g fiber/8oz and 1.9 NutraFlora for gut health
Kate Farms 1.5 Peptide – 1.5 Calories/mL – supposedly marketing for smaller tubes without needing to be watered down
Nutritional needs for burn patients
Calorie calculator is complex: https://burnstrauma.biomedcentral.com/articles/10.1186/s41038-017-0076-x/tables/1
2.5-4.0 g/kg/day protein for burned children vs 1.5-2.0 g/kg/day for adults
Fat should be less than 15% of total calories
Carbs 7g/kg/day for burned children
Where did swaddling begin and why do we do it? How do you swaddle a baby?
Etymology/History
- Swath (a strip in a field or a strip of cloth)
- 1325 first recorded use in English – Cursor Mundi (Gött.) l. 1343 A new-born child..Bunden wid a suadiling band (OED)
- Almost universal in the 18th century, with or without a cradleboard
Benefits of Swaddling (van Sleuwen, 2007)
- Infants arouse less and sleep more
- Soothes pain in infants
- Prevents hypothermia
- Decreases excessive crying due to stimulation
Adverse effects of swaddling (van Sleuwen, 2007)
- Hyperthermia if not monitored
- Increased risk of hip dysplasia
- Increased risk of SIDS if prone
- Promotes skin infections in hot, humid climates
Video showing three different methods of swaddling
Facial burns and airway management:
*The mortality associated with orofacial burns or smoke inhalation is related to the degree of lung damage, patient’s age, and the extent of the burn; it is not related to the method of upper airway control. Arch Surg. 1976
*In Facial burns, edema of the head and neck, supraglottic, and glottic areas is the most common cause of airway obstruction
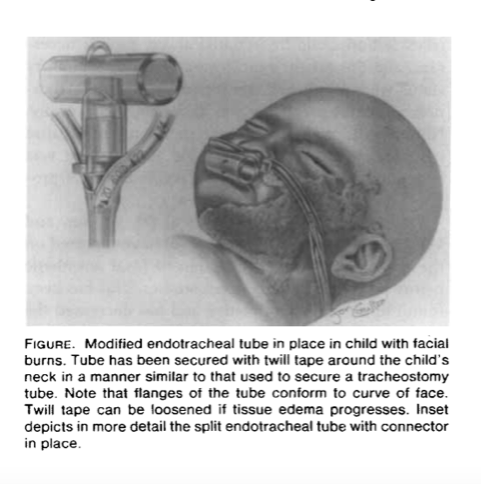
Modified Tube for Endotracheal Airway Management of Children with Facial Burns Antonio G. Galvis, MD,
The team from this article designed a particular ETT setup
Treatment for postextubation stridor was required after 11 (37%) of 30 extubations, with five reintubations and one tracheostomy. The best predictor of postextubation stridor was absence of an airleak at the time of extubation (sensitivity 100%, positive predictive value 79%, p less than .001), followed by type of injury (facial burn vs. all others; sensitivity 64%, positive predictive value 88%, p less than .001).
Kemper KJ, Benson MS, Bishop MJ. Predictors of postextubation stridor in pediatric trauma patients. Critical Care Medicine. 1991 Mar;19(3):352-355. DOI: 10.1097/00003246-199103000-00012. PMID: 1999096.
What a second line means!
The “second line” refers to the spectators who join or follow the main line (usually the brass band) and contribute to the walking parade. This is what separates a second line from any other New Orleans parade: groups are not only welcome but encouraged to follow along, allowing the second line to grow as it marches. The term “second line” doesn’t only refer to the parade itself, it also speaks to the type of dancing you will find during those parades. “Second lining” is a highly recognizable strutting, chicken-like dance move that many people use to keep pace with the band. So “second line” is a term with many meanings; it applies to a type of parade, a part of the parade, and a dance move used within that parade.





