
#Delight
Noticing things that delight you is a life changing practice that I first learned about reading Ross Gay’s work. (If you haven’t read any of his books, I’d start with The Book of Delights.)
And then there is 1000 Awesome Things, a blog that catalogues (as it promises!) awesome things that usually go unnoticed, but warrant celebration.

“Joy is an act of resistance.”
Toi Derricotte
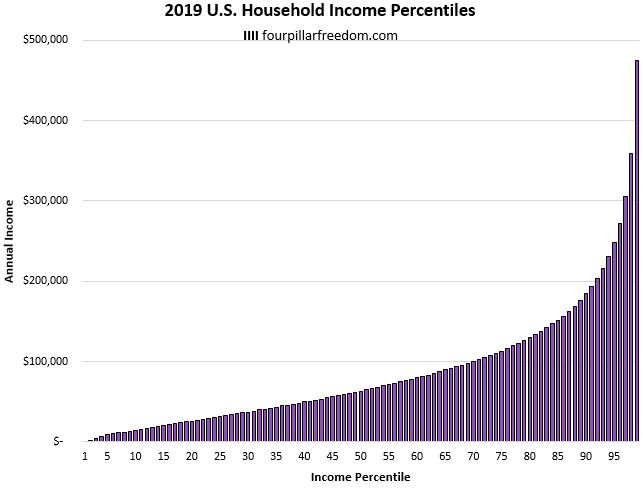
Scarcity is a choice, not a condition
The socioeconomic issues we face today aren’t new, so maybe it’s not a surprise that we struggle to even imagine a world where hunger, homelessness, and illness are faced with kindness and equity… which is why I was so intrigued with this article by Swapan Samanta, an economist who uses mathematics to understand social inequities.
“They [the prophets of five major religions] knew that food is never just food, that meals reveal the soul of a civilization, that the way we eat together – or fail to – determines whether we survive or collapse. Ancient wisdom and modern mathematics point to the same truth…Scarcity is a choice, not a condition.”

We can’t solve problems by using the same kind of thinking we used when we created them.
Albert Einstein
A reminder that today’s dogma is tomorrow’s history…
There was a beautifully designed study published this week that, for those of us who care (or have cared) for premature newborns is important.

For those not in medicine… the ductus arteriosus is a one of the necessary shunts around the lungs when babies are in the womb. (You don’t want blood going to the lungs which can’t oxygenate the blood because the baby isn’t breathing yet.) At the moment of birth, all that has to change… and pretty quickly. In term babies, it starts immediately, and the closure is done by 48-72 hours. In premature babies, it can take longer. And, in rare cases, it doesn’t close at all. When it stays open, we call it a patent ductus arteriosus (PDA).
Since the first surgical closure in 1938, PDAs have been closed by surgery, catheters, and medications. Over the last several decades there has been a progression in which way was the “right” way (and when it should be done). To summarize the overall trend, we began to move away from surgery and towards less invasive catheter and/or pharmacologic closure. Like all good research, there were lots of studies that preceded and led to the work published this week – which showed that just waiting (without medicines, surgery, or catheter closure) had the same outcome (a composite of death and/or bronchopulmonary dysplasia at 36 weeks) when compared to using medicines to close the PDA. Importantly, it also showed that the overall death rate was less in the babies who were just observed.
No difference in early death or lung disease, and a higher survival without any direct treatment.
This is why we do science.
This is why funding science is so very important.
p.s. Here’s another example of dogma becoming history… Surgically removing colons to cure schizophrenia. (😳)












{kind=link}