
When it comes to protecting your lower back as a surgeon it’s all about multifidus.
So says Professor Takuya Shimizu, an orthopedic surgeon and professor of sports science at Chukyo University who I heard speak at the 124th meeting of the Japanese Surgery Society.

I never learned about multifidus in anatomy class, and if you are a physician, I suspect you didn’t either. According to Wikipedia, “The multifidus (multifidus spinae : pl.: multifidi) muscle consists of a number of fleshy and tendinous fasciculi, which fill up the groove on either side of the spinous processes of the vertebrae, from the sacrum to the axis.”

I hope the experts forgive my “translation” of their expertise, but here is what I wish someone had told me about protecting my back (and decreasing back pain).
Anatomy. In the first year of medical school we learn about the large muscles that flex and extend the lower back – rectus abdominis anteriorly and the erector spinae posteriorly. Deep to these muscles are the muscles that stabilize the segments of the lumbar spine, and multifidus, for surgeons, is probably the most important of these muscles.
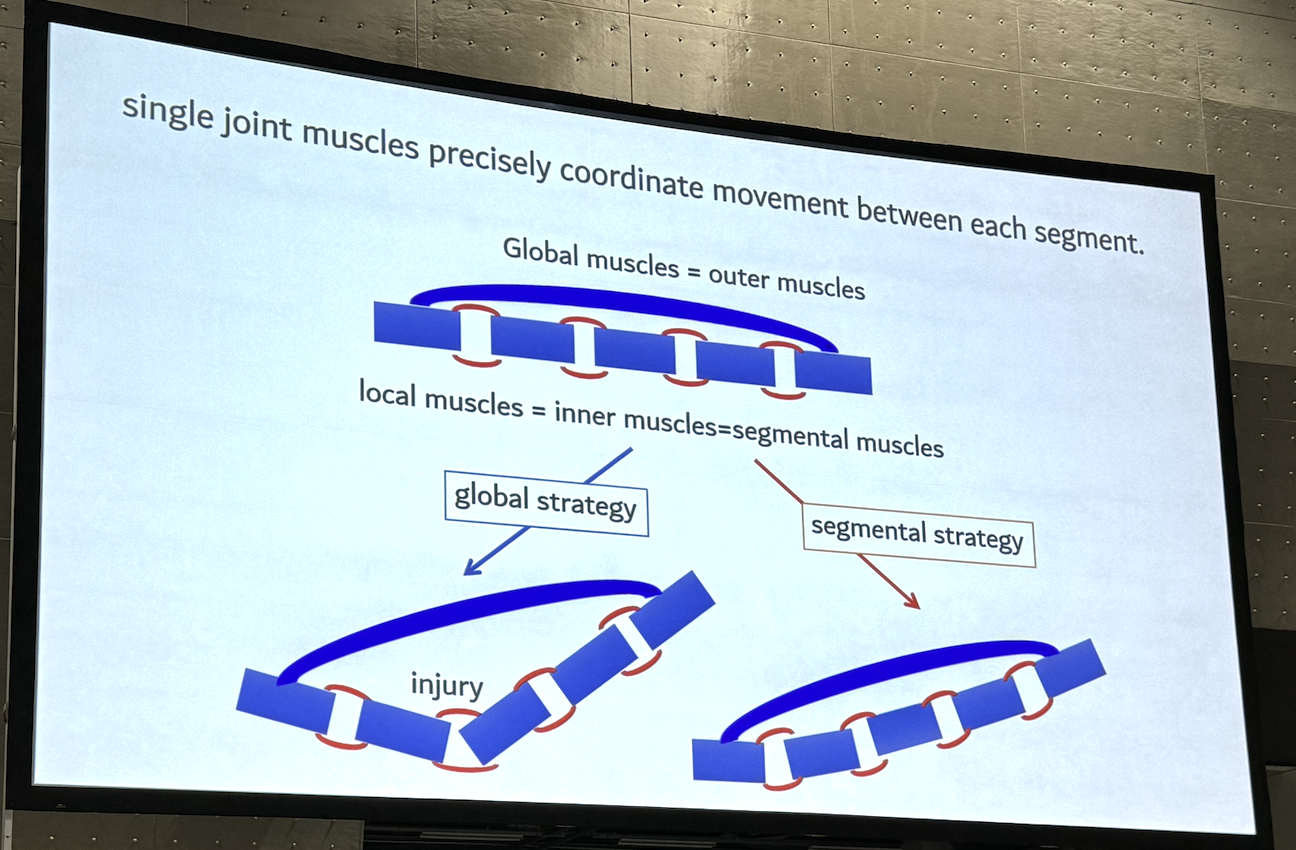
This is the slide from Dr. Shimizu that explained this in a way I could really understand. The “global” muscle in his slide is the rectus abdominis which we contract when we lean forward to operate or examine patients. If you have weak segmental muscles (i.e. the multifidus), a disproportionate force will be transmitted to the weakest point in the spine. For most people, that’s L5-S1. If you work to strengthen the multifidus (“segmental strategy”) the force generated with flexion will be distributed along all the vertebrae – which helps prevent pain and injury.
How to strengthen the multifidus.
“Walk like a model”… which is a conscious, three step process as explained by Dr. Shimizu. The goal should be to do this as often as you think of it (on rounds perhaps?) … and hopefully for 10,000 steps a day! (any amount helps, though)

There are also specific exercises you can do to strengthen the multifidus. The classic core exercises known as “bird dog” and “superman” are among the most effective. (Dafkou, 2021). Others that help include side planks, quadruped leg lift, and one arm pushup on a counter or bench. There are many more, so if you want a complete list, just google “multifidus exercises”.
Another excellent option is Pilates, which has been shown to be effective in strengthening deep core muscles and reducing low back pain. (Eliks, 2019). Tai Chi, yoga and other similar practices are effective in strengthening core muscles as well.

This amazing art is from the team at Codex Anatomicus… make sure you check out their website!
p.s. If you are a physical therapist, sports medicine expert, or have other expertise in this area, please comment below to add your expertise!
p.p.s If your back really hurts, please go see a good physical therapist.






















{kind=link}
{kind=link}